Can a mouthpiece treat sleep apnea?
Is a sleep apnea mouthpiece the same as a night guard?
Who is a MAD appropriate for?
Can you have both sleep apnea and bruxism?
Does Reviv treat sleep apnea?

For millions of people diagnosed with sleep apnea, CPAP is the gold standard. It works. But it’s also a machine that straps a mask to your face, generates continuous airflow, and requires nightly setup, cleaning, and a power source. Compliance rates for CPAP are notoriously low — studies estimate that between 30% and 50% of people prescribed it don’t use it consistently.
That gap — between what CPAP can do and what people will actually do — is where oral appliances enter the picture.
A mouthpiece for sleep apnea — clinically known as a mandibular advancement device, or MAD — is a custom-fitted oral appliance that repositions the lower jaw slightly forward during sleep. This forward positioning keeps the airway more open, reducing the collapse and obstruction that causes apnea events.
This article explains how oral appliances work, who they’re appropriate for, how they compare to CPAP, and what the important limitations are. It also explains the distinction between a sleep apnea device and a standard tooth-protection night guard — because these are different appliances with different regulatory clearances, and the difference matters.
What Is Sleep Apnea?
Sleep apnea is a condition in which breathing repeatedly stops and starts during sleep. The most common form — obstructive sleep apnea (OSA) — occurs when the throat muscles relax during sleep and the soft tissue partially or fully collapses, blocking the airway.
Each obstruction is an apnea event. Depending on severity, a person with OSA may experience dozens or hundreds of these events per night — each causing a partial arousal as the brain detects low oxygen and triggers resumed breathing.
The consequences of untreated sleep apnea can be significant: fragmented sleep, daytime fatigue, reduced cognitive function, and elevated cardiovascular risk over time. It warrants proper medical diagnosis and management.
| Severity | AHI | Description |
|---|---|---|
| Mild | 5–14 events/hour | Noticeable symptoms; first-line treatment options vary |
| Moderate | 15–29 events/hour | CPAP typically recommended |
| Severe | 30+ events/hour | CPAP strongly indicated; MAD less likely to be sufficient |
How CPAP Works
Continuous Positive Airway Pressure (CPAP) delivers a constant stream of pressurised air through a mask worn over the nose or mouth and nose. The air pressure acts as a pneumatic splint — it physically holds the airway open throughout the night, preventing collapse.
CPAP is highly effective when used correctly. For moderate to severe sleep apnea, it’s the benchmark against which other interventions are measured. The challenge is adherence: the mask, noise, required nightly setup, and sensation of pressurised airflow cause many people to abandon it.
How Oral Appliances Work for Sleep Apnea
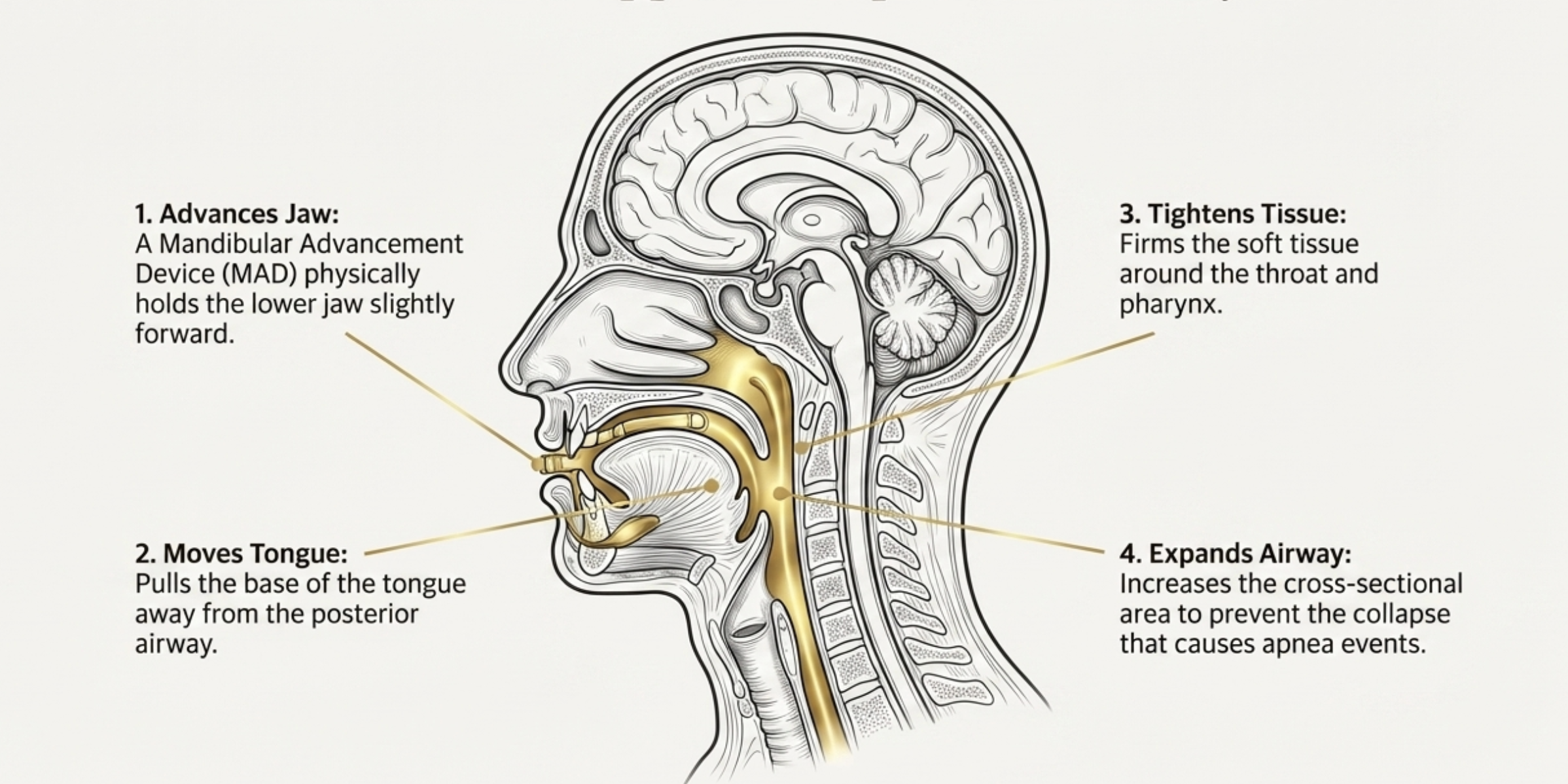
A mandibular advancement device (MAD) is a custom-fitted oral appliance that holds the lower jaw (mandible) in a slightly forward position during sleep. This forward positioning:
- Advances the tongue base away from the posterior airway
- Tightens the soft tissue around the throat and pharynx
- Increases the cross-sectional area of the upper airway
- Reduces the likelihood of airway collapse during sleep
The degree of advancement is adjustable in most clinical MADs — the dentist or sleep specialist titrates the device over several appointments, incrementally increasing the forward position until symptoms are adequately managed.
MAD vs CPAP: An Honest Comparison
| CPAP | Mandibular advancement device | |
|---|---|---|
| How it works | Pressurised air holds airway open | Jaw repositioning increases airway space |
| Effectiveness | High across all severity levels | Best for mild to moderate OSA |
| Compliance | Lower (mask, noise, setup) | Higher (small, silent, no power needed) |
| Side effects | Mask discomfort, dry mouth | Jaw soreness during adjustment period |
| Portability | Requires machine and power source | Compact, travel-friendly |
| Prescription | Yes | Yes |
| Cost | $500–$3,000+ (machine + supplies) | $1,500–$2,500 (dentist-fitted) |
MADs show comparable health outcomes to CPAP in mild-to-moderate patients — higher compliance compensates for slightly lower per-night efficacy.
Who Is a MAD Appropriate For?
Oral appliance therapy for sleep apnea is most appropriate for:
- Mild to moderate OSA — patients with severe OSA typically require CPAP
- CPAP intolerant patients — people who have genuinely tried CPAP and cannot tolerate it
- Positional OSA — sleep apnea primarily or significantly worse in the supine position
- Patients without severe jaw joint issues — MADs require sustained jaw protrusion
Who is not well-suited for a MAD: severe OSA, significant existing dental or jaw problems, central sleep apnea, or patients who grind heavily and need tooth protection rather than jaw repositioning.
Critical Distinction: A MAD Is Not a Night Guard
A mandibular advancement device for sleep apnea and a night guard for bruxism are fundamentally different appliances. They look similar. They both go in your mouth at night. But:
A MAD repositions the jaw — it holds the mandible forward to open the airway. This is a therapeutic action with specific medical intent. MADs for sleep apnea must be FDA-cleared as Class II medical devices. They require a sleep apnea diagnosis, a prescription, and professional fitting and titration.
A night guard protects teeth — it sits over the teeth and absorbs grinding force. A standard custom night guard is an FDA-registered Class I device designed for tooth protection. It does not reposition the jaw and has no indication for sleep apnea.
If you have both sleep apnea and bruxism — a common combination — you may need to discuss with your clinician which appliance takes priority, or whether a combination device is appropriate for your situation.
The Bruxism and Sleep Apnea Connection
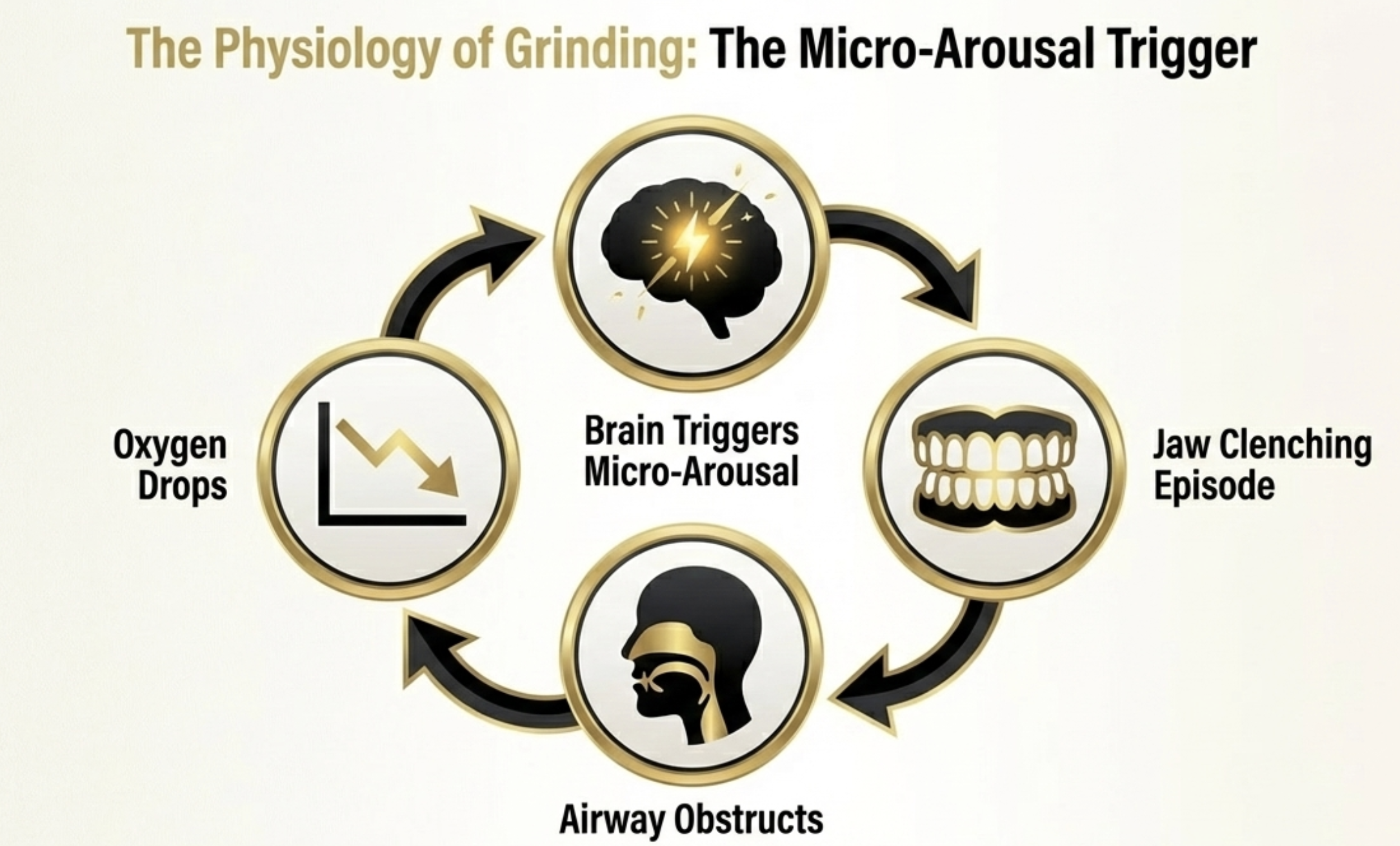
One reason this topic is relevant to a grinding and clenching audience: bruxism and sleep apnea co-occur at a notably high rate. Research indicates that people with obstructive sleep apnea have significantly elevated rates of sleep bruxism. The proposed mechanism involves micro-arousals — as the airway obstructs and oxygen drops, the brain triggers brief arousal events that can manifest as grinding episodes.
This means: if you’ve been diagnosed with sleep apnea, it’s worth discussing bruxism with your dentist. If you have confirmed bruxism, it may be worth discussing sleep apnea screening with your doctor. The two conditions often need to be managed in parallel.
Getting Diagnosed and Getting the Right Device
If you think you may have sleep apnea, the path is:
- See your doctor — describe your symptoms (snoring, witnessed apnea, daytime fatigue, unrefreshing sleep)
- Sleep study — either an in-lab polysomnography or a home sleep apnea test will measure your AHI and confirm diagnosis
- Treatment discussion — based on severity and your preferences, your clinician will recommend CPAP, MAD, positional therapy, or other interventions
- If MAD is recommended — you’ll typically be referred to a dentist with sleep medicine training for fitting and titration
- Discuss bruxism — if you also grind, raise it with both your doctor and dentist so both needs can be addressed
What to Look for in a Sleep Apnea Oral Appliance
If you’ve been prescribed an oral appliance for sleep apnea by a clinician, here’s what distinguishes a quality device:
- FDA clearance as a Class II device — specifically cleared for sleep apnea treatment (different from a Class I night guard)
- Custom fit — made from impressions of your teeth; one-size-fits-all MADs are significantly less effective
- Adjustable advancement — the ability to titrate the forward position incrementally is important for both efficacy and comfort
- Retention — the device must hold both arches securely; devices that allow the jaw to drop back lose their effect
- Durability — worn every night, the device needs to last; check materials and warranty
The Bottom Line
A mouthpiece for sleep apnea — a mandibular advancement device — is a legitimate, evidence-supported alternative to CPAP for mild to moderate obstructive sleep apnea. It works by repositioning the lower jaw to maintain airway space during sleep, offers high compliance compared to CPAP, and produces comparable health outcomes for appropriate patients.
It is not, however, a standard night guard. The two appliances serve different purposes, work by different mechanisms, and carry different regulatory requirements. If you need tooth protection from grinding, you need a night guard. If you need sleep apnea treatment, you need a clinician-prescribed MAD. If you need both — which is common — both need to be addressed with coordinated input from dental and medical professionals.
For anyone whose primary concern is protecting their teeth from grinding pressure during sleep, the Reviv how-to-choose guide is the right starting point — or browse the full range of FDA-registered Class I appliances designed for tooth protection. For sleep apnea, please speak with your doctor.