What is the best CPAP alternative?
Can you treat sleep apnea without CPAP?
Is a MAD as good as CPAP?
Can positional therapy treat sleep apnea?
Does Reviv treat sleep apnea?

CPAP works. That’s not in question.
For moderate to severe obstructive sleep apnea, continuous positive airway pressure remains the most effective treatment available. When worn consistently, it virtually eliminates apnea events, improves sleep quality, and reduces the long-term health consequences of untreated sleep apnea.
The problem is the word “consistently.” Studies put CPAP non-compliance rates at 30–50%. Masks leak. Noise disturbs partners. Some people find the sensation of pressurised airflow suffocating rather than helpful. Travel is complicated. The machine requires a power source and nightly disassembly for cleaning.
For the millions of people who genuinely cannot tolerate CPAP — despite trying different masks, pressure settings, and adjustment periods — alternatives are not a cop-out. They are a legitimate and clinically recognised part of sleep apnea management.
Why CPAP Compliance Is Such a Problem
Before looking at alternatives, it’s worth understanding why CPAP fails so many people — because the alternative chosen should address the specific reason CPAP didn’t work.
Common reasons for CPAP non-compliance:
- Mask discomfort or pressure sores
- Claustrophobia or feeling of suffocation
- Noise from the machine or airflow
- Difficulty exhaling against positive pressure
- Dry mouth or nasal congestion
- Disruption to bed partner
- Travel inconvenience and power requirements
- Psychological resistance to the identity of “CPAP user”
Some of these are addressable within CPAP itself — different mask types, pressure relief settings, heated humidifiers, travel-sized machines. Before concluding CPAP isn’t workable, it’s worth exhausting these options with a sleep specialist.
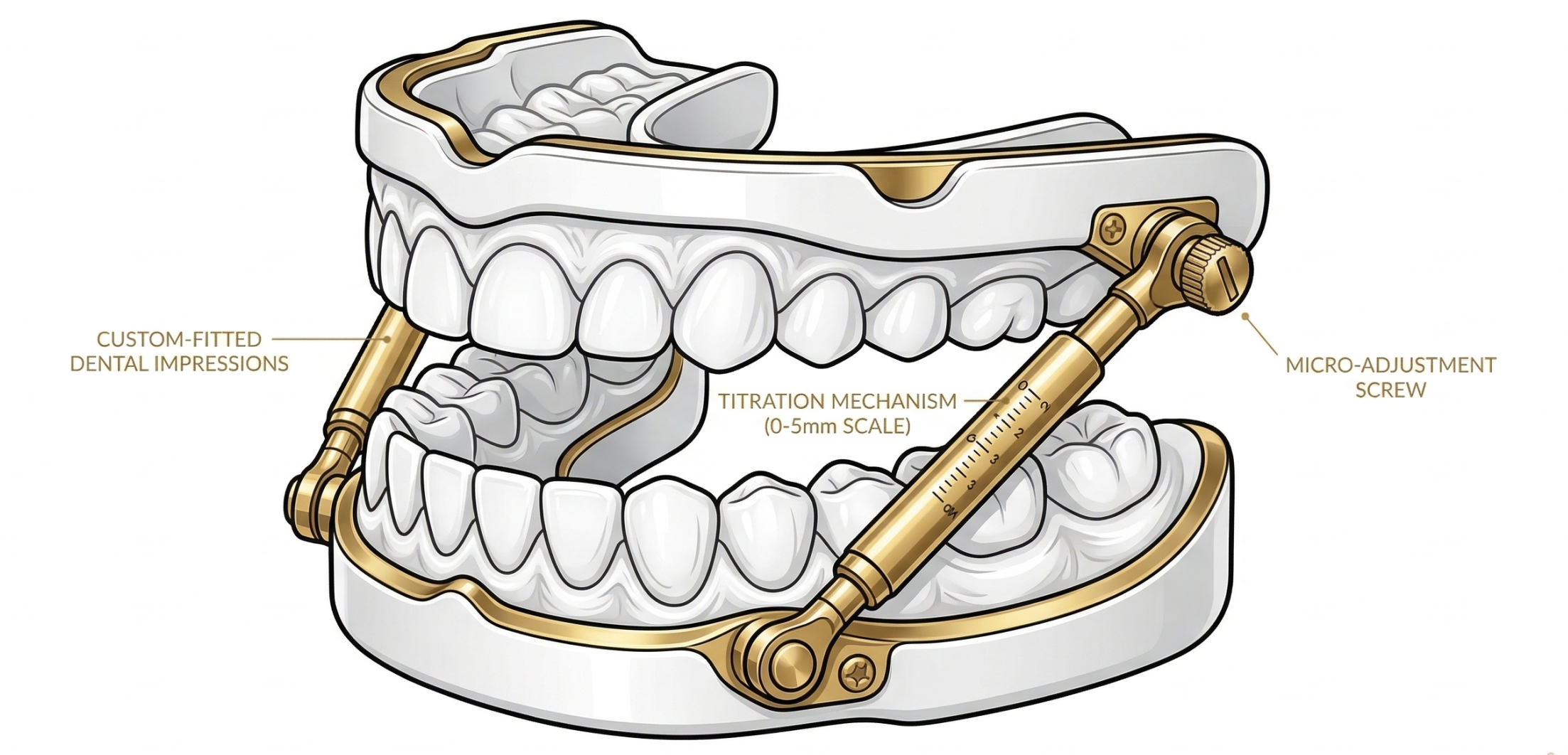
1. Mandibular Advancement Device (MAD)
A custom-fitted oral appliance that holds the lower jaw slightly forward during sleep. This forward positioning advances the tongue base away from the airway, increases airway cross-section, and reduces the collapse that causes apnea events.
Evidence: MADs are the most evidence-supported CPAP alternative for mild to moderate OSA. While CPAP typically produces greater AHI reduction per night, MADs often achieve comparable health outcomes because compliance is significantly higher.
Best for: Mild to moderate OSA; CPAP-intolerant patients; frequent travellers; those who prefer a smaller, non-powered device.
Not suitable for: Severe OSA (AHI 30+) in most cases; significant TMJ disorder; very limited jaw mobility; poor dentition.
Requires: Clinician diagnosis; dentist with sleep medicine training for fitting; iterative titration appointments.
2. Positional Therapy
Interventions that prevent sleeping in the supine (back-sleeping) position. For many people with OSA, apnea events are significantly more frequent when lying on their back — gravity pulls the tongue and soft palate into the airway. Positional therapy keeps the person on their side throughout the night.
Approaches range from simple (a tennis ball sewn into the back of a sleep shirt) to purpose-built devices (vibrating positional alarms worn on the chest that alert the sleeper when they roll onto their back).
Evidence: Well-supported for positional OSA — where AHI in the supine position is at least twice the AHI in the lateral position. For non-positional OSA, it’s less effective.
Best for: Confirmed positional OSA; mild to moderate severity; those who find other interventions difficult to tolerate.
3. Upper Airway Surgery
Surgical procedures that physically alter the anatomy of the upper airway to reduce the likelihood of collapse. Options include uvulopalatopharyngoplasty (UPPP), tonsillectomy (where enlarged tonsils are a contributing factor), and various soft tissue or skeletal procedures.
Evidence: Surgical outcomes for OSA are variable and depend heavily on the specific anatomy driving the obstruction. UPPP has modest success rates overall, but targeted procedures in appropriately selected patients can be effective.
Best for: Patients with specific anatomical contributors; those who have failed other treatments; selected by a specialist after comprehensive assessment.
Not suitable for: As a first-line treatment; without specialist ENT or sleep surgeon evaluation.
4. Weight Management
Intentional reduction of excess weight, particularly in the upper body and neck. Excess weight around the throat increases the likelihood of airway collapse during sleep. Significant weight loss can meaningfully reduce OSA severity in people whose sleep apnea is substantially driven by excess weight.
Evidence: The relationship between obesity and OSA is well-established. Studies show that significant weight loss can produce clinically meaningful reductions in AHI. In some cases of mild to moderate OSA in obese patients, weight normalisation has reduced AHI to sub-clinical levels — though this is not universal.
Best for: OSA patients with obesity as a contributing factor.
Not suitable for: As a standalone intervention for moderate to severe OSA while waiting for weight loss; patients without significant excess weight.
5. Inspire Therapy (Hypoglossal Nerve Stimulation)
A surgically implanted device that stimulates the hypoglossal nerve — which controls tongue movement — to keep the tongue from falling back into the airway during sleep. The device monitors breathing patterns and delivers mild electrical stimulation in sync with each breath.
Evidence: Clinical trials show significant AHI reduction for appropriate candidates. Inspire has FDA approval for moderate to severe OSA in CPAP-intolerant patients who meet specific anatomical and clinical criteria.
Best for: Moderate to severe OSA; CPAP-intolerant patients who meet anatomical criteria (determined by sleep endoscopy); those who are surgical candidates.
Not suitable for: Complete concentric palatal collapse; non-surgical candidates; mild OSA.
6. Nasal Devices and Airway Support
A range of non-invasive devices designed to improve nasal airflow and reduce mouth breathing during sleep. These include nasal dilator strips, internal nasal dilators, and nasal expiratory positive airway pressure (EPAP) devices that create resistance on exhale to maintain airway pressure.
Evidence: Nasal strips have limited evidence as standalone sleep apnea treatments but can improve nasal breathing. EPAP devices have more evidence — studies show meaningful AHI reduction in mild to moderate OSA for some patients.
Best for: Mild OSA; nasal congestion contributors; low-cost non-invasive adjuncts.
Not suitable for: Moderate to severe OSA as standalone treatment.
7. Lifestyle Interventions
Modifications to sleep habits and lifestyle factors known to worsen OSA. Key interventions include:
- Alcohol avoidance before sleep — alcohol relaxes pharyngeal muscles and significantly worsens airway collapse
- Sedative medication review — some medications relax airway muscles; reviewing these with your prescriber may help
- Exercise — independent of weight loss, exercise has been shown to reduce OSA severity, possibly through effects on upper airway muscle tone
- Sleep hygiene improvements — consistent schedule, cool bedroom temperature, optimised sleep environment
Evidence: Supported as adjuncts to primary treatment rather than standalone solutions for moderate to severe OSA. Alcohol avoidance in particular has a well-documented acute effect on apnea severity.
Comparing the Alternatives
| Alternative | Evidence | Best severity | Invasiveness |
|---|---|---|---|
| Mandibular advancement device | Strong | Mild–moderate | None |
| Positional therapy | Moderate | Positional OSA | None |
| Surgery (UPPP etc.) | Variable | Case-dependent | High |
| Weight management | Strong (where relevant) | Mild–moderate | None |
| Inspire (nerve stimulation) | Strong (in candidates) | Moderate–severe | Surgical |
| Nasal devices / EPAP | Moderate | Mild | None |
| Lifestyle interventions | Moderate (as adjuncts) | All levels | None |
The Bruxism and Sleep Apnea Overlap
Sleep apnea and bruxism co-occur at a notably elevated rate. Research indicates that people with OSA show significantly higher rates of sleep bruxism than the general population. The proposed mechanism involves micro-arousals — as the airway obstructs, the brain arouses briefly to resume breathing, and this arousal can manifest as a grinding episode.
This means: if you have confirmed bruxism, it may be worth discussing sleep apnea screening with your doctor — particularly if you snore, feel unrefreshed after sleep, or have a bed partner who has noticed breathing pauses. Conversely, if you’re being managed for sleep apnea, tooth protection during sleep is worth discussing with your dentist.
The Bottom Line
CPAP remains the most effective treatment for sleep apnea — but for people who genuinely cannot tolerate it, several evidence-based alternatives exist. The mandibular advancement device has the strongest evidence base among non-surgical alternatives for mild to moderate OSA. Positional therapy, weight management, and lifestyle modifications are useful adjuncts. Inspire therapy offers a surgical option for appropriate severe OSA patients who are CPAP-intolerant.
The right alternative depends on your specific OSA severity, anatomy, and circumstances — and should be determined with a qualified sleep clinician, not chosen independently. If you’re managing bruxism alongside sleep apnea, your dentist is the parallel conversation.