

What causes snoring?
How do I stop snoring?
Is snoring a sign of sleep apnea?
Do nasal strips help snoring?
Does alcohol cause snoring?

Almost everyone snores at some point. Across a cold, after a few drinks, during a particularly deep sleep — the sound is familiar. For many people though, snoring is not occasional. It’s nightly, loud, and affecting both their own sleep quality and their partner’s.
Understanding what causes snoring is the first step to addressing it. Snoring isn’t one problem with one fix — it’s a symptom that can come from several different causes, each of which responds to different interventions. The person snoring because of nasal congestion needs a different solution than the person snoring because of sleep position, excess weight, or a relaxed soft palate.
What Is Snoring, Exactly?
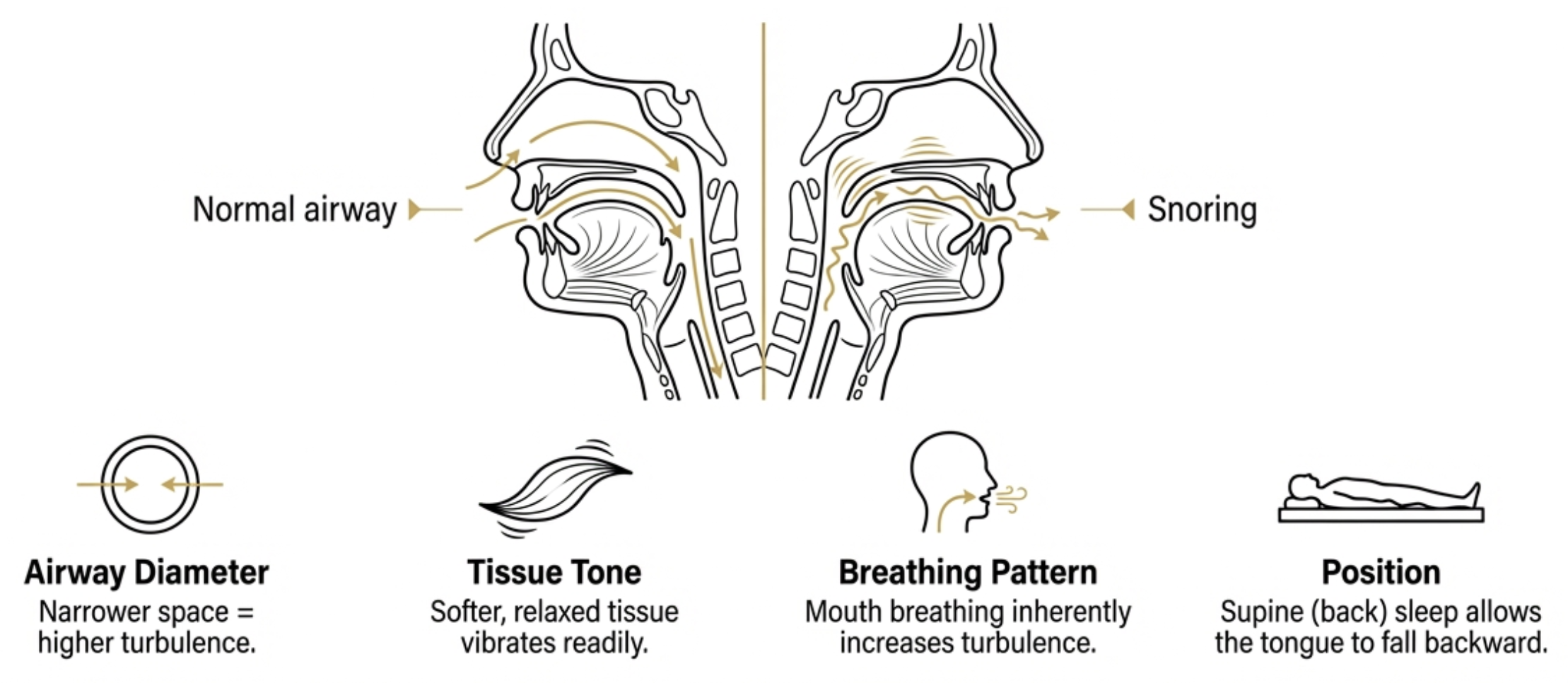
Snoring is the sound produced when airflow causes the tissues of the upper airway to vibrate. During sleep, the muscles of the throat, tongue, and soft palate relax. As air moves through the narrowed airway, the soft tissue flutter and vibrate — producing the characteristic sound that ranges from a gentle rumble to a loud, disruptive noise.
The key variables are airway diameter (narrower = more turbulence and vibration), tissue tone (softer, more relaxed tissue vibrates more readily), breathing pattern (mouth breathing produces more turbulence), and sleep position (supine sleep allows the tongue and soft palate to fall backward into the airway). Almost any factor that narrows the airway, reduces tissue tone, or promotes mouth breathing can contribute to snoring.
The 8 Most Common Causes of Snoring
1. Sleep position — particularly sleeping on your back
In the supine position, gravity pulls the tongue and soft palate backward toward the throat, partially obstructing the airway. Many people who snore only on their back are classified as positional snorers — and for this group, side sleeping can dramatically reduce or eliminate snoring. Methods range from a body pillow to purpose-built positional alarm devices that vibrate when the wearer rolls supine.
2. Nasal congestion and obstruction
When nasal passages are congested — from a cold, allergies, sinusitis, or a deviated septum — airflow resistance increases and mouth breathing follows. Temporary congestion causes temporary snoring. Structural obstruction (deviated septum, polyps, enlarged turbinates) causes persistent snoring that needs ENT assessment. Nasal strips physically widen the nasal passages, reducing resistance — a simple first step for nasal-related snoring.
3. Alcohol and sedatives
Alcohol relaxes the pharyngeal muscles more than normal sleep relaxation does, making the airway more flaccid and prone to collapse. Even moderate evening drinking meaningfully increases snoring frequency and intensity. The effect is dose-dependent and applies equally to benzodiazepines and sedating antihistamines. Reducing or eliminating alcohol in the 3–4 hours before sleep is often the highest-impact single change for alcohol-related snorers.
4. Excess weight around the neck
Adipose tissue around the neck narrows the airway at rest, increases the tendency of tissue to collapse under breathing pressure, and adds weight that gravity pulls inward during supine sleep. Neck circumference is a well-established predictor of snoring severity. Even modest weight loss can meaningfully reduce snoring in people where excess weight is a significant contributor.
5. Mouth breathing
Breathing through the mouth creates more turbulent airflow over the soft palate and uvula than nasal breathing, and delivers drier, more irritating air to throat tissues. Mouth breathing can be the primary cause of snoring, or a secondary effect of nasal obstruction. Addressing the nasal issue often resolves both. For habitual mouth breathers with clear nasal passages, nasal strips and mouth taping are the relevant interventions.
6. Anatomy — palate, uvula, and jaw structure
A long or thick soft palate or uvula vibrates more readily during sleep. A naturally narrow pharynx increases turbulence. Retrognathia (recessed jaw) positions the tongue base closer to the posterior airway, increasing narrowing. Enlarged tonsils or adenoids — particularly in children — are a significant cause of snoring. Anatomical factors are not addressable without clinical intervention and explain why some people snore despite doing everything “right” with lifestyle.
7. Age
Muscle tone throughout the body decreases with age — including the pharyngeal muscles. As these muscles lose tone, the airway is more prone to partial collapse during sleep. Age-related snoring itself isn’t reversible at root, but its secondary contributors (weight, alcohol, position, nasal patency) remain modifiable.
8. Nasal polyps and chronic sinusitis
Unlike intermittent cold or allergy congestion, nasal polyps and chronic sinusitis cause continuous nasal obstruction that doesn’t resolve with time. Medical management with intranasal corticosteroids or ENT assessment is the appropriate approach. Nasal strips may provide partial symptomatic relief while addressing the underlying condition.
Snoring vs Sleep Apnea: An Important Distinction
Simple snoring involves vibration of upper airway tissue without complete obstruction. Breathing continues uninterrupted; no significant oxygen drops or arousal events.
Obstructive sleep apnea (OSA) involves complete or near-complete airway collapse during sleep, causing breathing to stop repeatedly. These events cause oxygen desaturation, sleep arousal, and significant disruption to sleep architecture — with cardiovascular implications that simple snoring does not carry.
| Simple snoring | Obstructive sleep apnea | |
|---|---|---|
| Airway | Narrowed but open | Collapses completely |
| Breathing | Continuous | Stops repeatedly |
| Oxygen levels | Normal | Drops during events |
| Health implications | Primarily social/partner | Cardiovascular, metabolic |
| First step | Lifestyle intervention | Medical assessment |
Practical Interventions by Cause
| Cause | First-line approach | If first-line fails |
|---|---|---|
| Supine sleep position | Side-sleeping, body pillow | Positional alarm device |
| Temporary nasal congestion | Saline rinse, humidifier, nasal strips | Short-term decongestant |
| Structural nasal obstruction | Nasal strips, ENT assessment | Surgical correction |
| Alcohol / sedatives | Reduce evening consumption | Full lifestyle review |
| Excess weight | Weight management programme | Concurrent lifestyle changes |
| Mouth breathing | Nasal strips, mouth taping | Address underlying nasal cause |
| Anatomical factors | ENT assessment | Surgical / MAD options (clinical) |
| Nasal polyps / sinusitis | Medical management | ENT referral |
The Bruxism and Snoring Connection
For readers managing teeth grinding or jaw tension, there’s a relevant overlap: bruxism and snoring frequently co-occur, often because of shared underlying factors. Both conditions are associated with sleep-disordered breathing, arousal during sleep, and sleep apnea. The micro-arousals triggered by apnea events are associated with grinding episodes; the same apnea events often drive snoring.
This means: if you snore significantly and also grind your teeth, mention both to your doctor and dentist. If you’re being assessed for sleep apnea, raise tooth protection simultaneously. And if you already wear a night guard for grinding — it doesn’t address snoring. The two problems need separate approaches.
The Bottom Line
Snoring is caused by airway narrowing and tissue vibration — but the specific driver varies significantly between individuals. Sleep position, nasal obstruction, alcohol, excess weight, mouth breathing, and anatomy each contribute differently and respond to different interventions. The most effective approach starts with identifying your primary cause.
If snoring is accompanied by witnessed breathing pauses, morning headaches, or significant daytime sleepiness, sleep apnea assessment takes priority over all lifestyle interventions. For nasal airflow support, browse Reviv nasal strips — or for anyone managing both snoring and nighttime tooth grinding, explore the full Reviv range of FDA-registered Class I oral appliances.

